"He isn't deaf........but he can't hear"
Now,a month after learning that Jake was hearing impaired, we found ourselves in the audiology lab at Louisiana State University Medical School with Charles I. Berlin, Ph.D., the director of the Kresge Hearing Research Lab of the South. We discovered that we had been referred to him because Jake's test results didn't appear to be those of a "typical deaf child". I'll never forget that day, February 15, 1995, the first day we heard mention of the term Auditory Neuropathy. It wasn't until later we knew how fortunate we were to live in the area and be able to see Dr. Berlin with a one day notice.
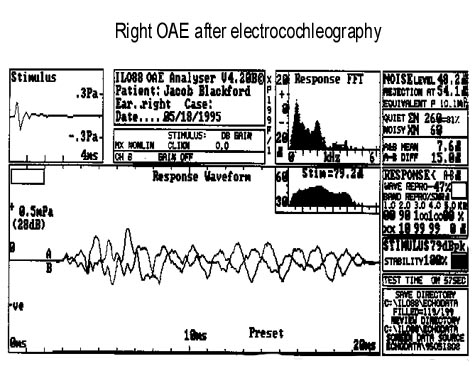
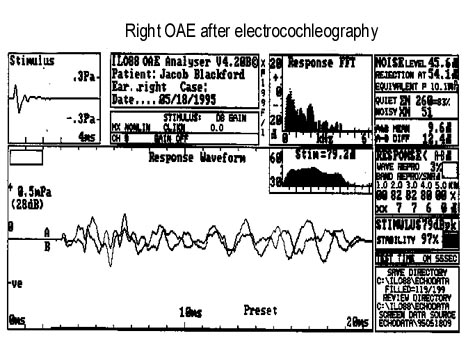
Because auditory neuropathy was suspected, he would need to have another ABR with positive and negative polarity clicks. We attempted to do another ABR that first day but Jake started to wake up about ten minutes into the test and kept thrashing his head about and whimpering. We tried anything and everything to get through the testing without success. We were able to get a quick screen otoacoustic emissions (OAE's) from his right ear before he woke up. The OAE's were present and robust. This meant that his cochlea was functioning at the outer hair cell level. In other words, that he wasn't deaf even though he acted deaf.
For three months we had tried to obtain complete ABR and OAE results, but each time Jake was given Chloral Hydrate, the amount of time he slept grew shorter. By the third attempt at sedation, he didn't even go to sleep. He was so aggitated, crying, screaming, kicking and trying to bite that I couldn't control him. He wanted to walk but was so drunk he couldn't stand. I started to cry because I couldn't handle him anymore. At that point, Dr. Berlin took him out into the hall and tried to calm him but you could hear him screaming all over the Kresge lab. The amazing part is that when they came back in and Dr. Berlin played the keyboard, Jake got quiet and sat there calmly. Either he heard some of the music or felt the vibrations. We weren't sure which.
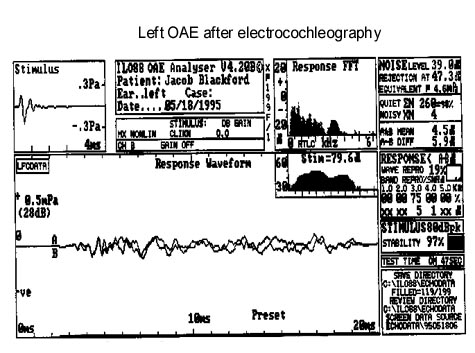
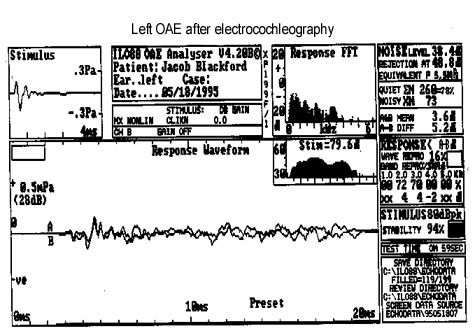
Finally, after the months of trying to get the results we needed, we found that "Jake doesn't sedate" and decided that he should undergo general anesthesia in order to obtain accurate and complete results. In May it was all in black and white. We had all the results we could ever need. He had OAE's testing, an ABR and electrocochleography. The report read as follows:
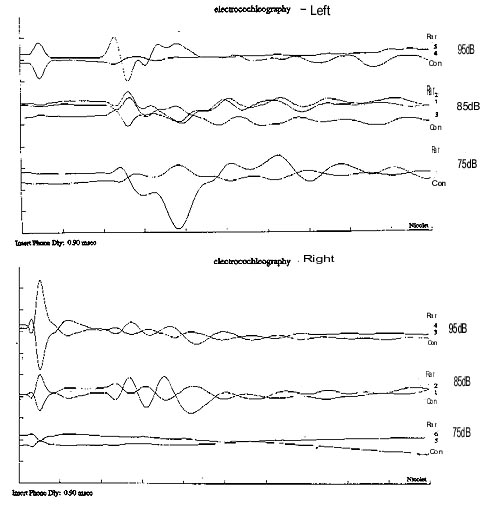
We also performed a transtympanic electrocochleogram which confirmed that he has normal outer hair cell function but inverted responses based on the polarity of the stimulus. This is inconsistent with intact auditory nerve synchrony. It is possible that he has a detached tectorial membrane or related mechanical pathology that isolates mechanical from neural stimuli.
I remember Dr. Berlin coming out to the waiting room and telling us that Jake isn't deaf....but he can't hear. We officially had the diagnosis of Auditory Neuropathy. He had present OAE's but they were not normal which signified a probable sensorineural hearing loss with the auditory neuropathy. So he wasn't a "typical auditory neuropathy" child either.
After the testing, we learned that some cases of auditory neuropathy have been linked to systemic neurological disorders like Charcot-Marie-Tooth Syndrome. And we learned that an absent ABR can show if there is a problem with the brainstem, other neural ear structures,the possibility of an absent auditory nerve, or tumors blocking the nerve. With these possibilities on the table, we were referred to a pediatric neurologist. After a battery of physical tests, his impression was that Jake was a "normal developing sixteen month old with an unusual hearing loss of unknown pathology with no signs of systemic neuropathy." To rule out the possibility of acoustic tumors, absence of the auditory nerve or other pathological problems Jake needed an MRI of the brain and auditory apparatus. The next week we were having yet another test that he had to be sedated for. I scheduled it for his nap time and kept him up most of the night before with the hope that he would sleep for the test. After the medication to sedate him was given, my prayers were answered when he slept long enough to allow the doctors to complete testing.
He looked so small and helpless inside that huge machine; it was difficult to think about what the worst case scenario could be, so I tried to shut the thoughts out of my mind. After the test, the radiologist told us that the neurologist would be in contact with us in a few days to explain the results. I knew I would be crazy waiting a few days. The department nurse told the MD that I am a nurse, so he showed me the films. He explained that all the structures were present and there were no tumors or malformations. He saw no reason for Jake's hearing loss on the MRI. The MRI completed the testing phase and it was official, Jake had auditory neuropathy.
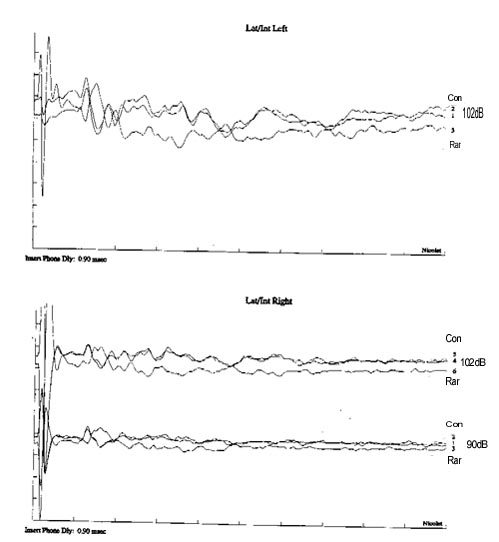
When studied by ABR he appears to be deaf if an alternating polarity pulse is used and therefore could have been misdiagnosed as being peripherally deaf; however, the original referring agents quite correctly were concerned about the nature and significance of the data they obtained. We found Jacob to have normal hair cell emissions, meaning that the outer hair cells and middle ear are functioning normally. His ABR would have been absent if collected to alternating polarity clicks, but is consistent with undamped cochlear microphonics when collected with clicks of opposite polarity.
 Jake's hair stood on end for months after he had general anesthesia. They told us it couldn't be the anesthesia, but it didn't look like this before. It wasn't like we would sue them for "bad hair secondary to anesthesia." (smile). It was a glowing blond color and we got plenty of strange looks from people everywhere we went. We tried Frizz-Ease after months of searching for something to make it stay down. It helped some, but finally as his hair grew back it would lay down!
Jake's hair stood on end for months after he had general anesthesia. They told us it couldn't be the anesthesia, but it didn't look like this before. It wasn't like we would sue them for "bad hair secondary to anesthesia." (smile). It was a glowing blond color and we got plenty of strange looks from people everywhere we went. We tried Frizz-Ease after months of searching for something to make it stay down. It helped some, but finally as his hair grew back it would lay down!